(A Rough Guide to Ireland – Part 1)
So you’re pregnant and you don’t want to be. What next? First things first – commiserations on finding yourself in this situation. It’s shit and it might get a bit worse before it gets better, but there are people out there who are rooting for you and hopefully you find the information in here a little bit useful. This is basically a step by step guide to getting through this situation.

Are you definitely definitely definitely pregnant?
Take a test. You can buy them in every pharmacy and they cost between €10/€20. Sometimes they sell them really cheap in Dealz and sometimes other pound shops for around €1.50/€2. If you’re embarrassed about buying it or worried someone might see you, consider asking a trusted friend to go and buy it for you. If you’re worried about what the shop assistant might think, just try and look excited. The chances are the sales assistant is selling these every day and will not pay any heed to you anyway. If you’re not sure about the home test you took, the IFPA carry out testing for €20 but it’s free if you have a medical card. Cura and Sexual Health Centre in Cork offer free pregnancy testing. Having an early scan so you can figure out how far along you are might be useful if you aren’t sure. You can get a free scan at FemPlus in Dublin and there are places around the country offering scans at a variety of locations with an average cost of around €100. The Abortion Support Network can tell you where the best place to go for a scan is. A scan will also confirm that the pregnancy isn’t ectopic. If you can’t get to a scan or afford a scan the most important thing when determining how far along you are is that you need to be counting from the first day of your last menstrual period, not from when you had sex.
Marie Stopes Reproductive Choices will provide you with a consultation and a scan but where they will charge €110 (or €90 for a phone consultation). It’s important to note that Marie Stopes’ clinics in Britain absolutely will not perform a procedure if you do not have the correct payment for it.
Decide if counselling is for you
Perhaps you’ve made a decision not to continue your pregnancy, or maybe you feel you want to chat confidentially about that decision with someone else. Here are a list of clinics that are legit crisis pregnancy clinics. The IFPA section about their counselling service has some useful links and shows the locations where they provide services around Ireland. When you go to these counselling services in those links, the counsellor is legally obliged to tell you about your options including parenting and adoption. Remember, whether or not you continue your pregnancy is your choice, and you need to do what’s right for you.
Be aware that there are other unethical “crisis pregnancy” services out there that are designed not to assist women but to push their anti-choice agenda.
You might not want to go to counselling, but bear in mind that it’s free and if you go to counselling with either Irish/ Northern Irish FPA, Well Woman, Femplus Clinics, One Family, Cork Sexual Health or here2help, and subsequently attend BPAS for a termination, you won’t have to pay the €80/€90 counselling fee that BPAS charge. A letter from the IFPA to say you attended counselling will waive the counselling fee charged at *any* English clinic.
There are lots of women who make their decision the second they find out they’re pregnant. There are lots who take some time to decide on their own. There are others who go to counselling. Do what works for you – but as soon as you make your decision to have an abortion, start the ball rolling on making the appointment.
So you’ve made a decision to have an abortion, what now?
How you proceed in accessing an abortion from here on, really depends on how much access to money you have. If you have money you can travel overseas to access termination services, and I’ll go into the logistics of this later. If you don’t have money to travel, there are still options.
The Abortion Support Network are an organisation that offer practical, non-judgemental information and advice, financial help and, when needed, accommodation in volunteer homes. They provide guidance on what is the cheapest way for you to have your abortion, and which clinics will be the best choice for you. Ring them before you make any appointment and travel plans. If it is a particularly busy time of year for UK clinics it may be cheaper and quicker for you to travel to the Netherlands or Brussels for your treatment (although you will definitely need a passport to travel there from Ireland). ASN has a network of volunteers in UK cities that will provide accommodation and meals for those who need or want to stay overnight – most women are able to travel in and out in one day.
The Abortion Pill
Abortion is illegal in almost all cases here so many women who don’t have the money to travel (or it simply is not an option for them because of their immigration status or relationship status or age or childcare arrangements) will illegally order the abortion pill from Women Help Women. The abortion pill is a safe medicine.
Some women in the 26 Counties have found that when they ordered this online that it was confiscated by Customs but to our knowledge, nobody has been prosecuted for attempting to receive pills online. In the 6 Counties however, there have been prosecutions for attempting to procure a miscarriage (there are criminal penalties for this in both jurisdictions). There are difficulties in ordering online, but it isn’t impossible. The medication is usually supplied in exchange for an €80 donation. Need Abortion Ireland help women access medications from Women Help Women.
Women on Web are another organisation that can sometimes deliver to Ireland. The organisation ROSA have twice partnered with Women on Web to drive a bus around Ireland to do consultations for pills and then the pills will be posted to you a few days later. This is worth noting if you’re using resources to travel to a place where the bus is going to be because they will take around 3 days to get them to you. It may be quicker to just order them online in many cases as Women Help Women take around 5 days delivery. Both Women Help Women and Women on Web are reputable providers of early medical abortion pill. However we understand that Women Help Women is faster to respond to client emails. There is another reputable provider of pills, called Safe2Choose, but they are not currently sending pills to the Republic of Ireland.
Both Women Help Women and Women on Web will ask you for a Northern Irish address in addition to your home address, or the address of the place you will be receiving the pills. If you do not have a friend in Northern Ireland, fill out the medical consultation and WHW or WOW will follow up with you.
Please do not attempt an abortion with any other remedy, herbal or otherwise, as you could inflict serious injury on yourself. While Women on Web and Women Help Women are trusted providers of the abortion pill, there is always a risk when buying medicine online when it comes from a source that isn’t trusted.
A safe place to have your abortion
Once you’ve got your pills, you’ll need a safe space to take them. Most people will do that at home but for some that won’t be an option so they might go to a trusted friend’s house. Need Abortion Ireland’s site provides useful advice and self-care tips for when you’re having your abortion. They also provide care packages and a text message support service 089 490 2517 available 6pm – 9pm, 7 days a week. You can email them at info@needabortionireland.org The British Pregnancy Advisory Service (BPAS) also provide a hotline for those living in Ireland with medical questions/concerns about medical abortion pills. BPAS can be reached at 1800 910 049 (ROI) and 0800 077 6049 (NI). Here are some tips on what to do if you think you’re in an emergency medical situation.
Increasingly, there appears to be a clampdown in the North on women taking the abortion pill, and a tendency towards prosecutions. Two prosecutions have been brought because someone touted on their housemate, and another two were reported by doctors. You are legally allowed to travel (if your immigration status is regularised) so telling your doctor you’re pregnant, or having them perform a pregnancy test should not be an issue. You do not have to tell them that you intend to have an abortion.
The Money
Figuring out how to pay for it, whether it’s the €80 donation for Women Help Women or €450 to a clinic and another €300 for flights, can be the most traumatic aspect of this experience for many women. If you are purchasing pills from Women Help Women or Women on Web and do not have the full requested donation, they may be willing to accept a smaller donation amount. If you’re later on in the pregnancy, or decide to travel to England, your procedure will cost more. The Abortion Support Network can help you with this but you may not wish to ask for that assistance. If you’re low on phone credit, you can request a call-back from the abortion clinics. Here is a list of clinics.
Many women take loans from their local Credit Union to fund their abortion. Generally speaking, they will let you borrow twice what you have in savings if a guarantor will sign for it. If you don’t have someone who can act as guarantor, you may need to get a student loan in a bank, or check if you can activate an overdraft facility on your account. Each credit union has different rules so it’s best to ask the branch you’re a member of. If you are in receipt of a social welfare payment you might be eligible to join and borrow from your local credit union through the Personal Microfinance Scheme. This was a government scheme introduced to try and stop people going to illegal money lenders. Try to avoid going to the illegal moneylenders at all costs. You could also go to the Community Welfare Officer to ask for an emergency payment. Keep in mind though that you will need to provide a reason why you need this payment, and if you say it is for a washing machine there is a chance you will need to either provide proof you purchased a washing machine or an inspector may call to check your purchase. You could take a chance and tell the CWO why you need the payment as they have a wide range of discretion but you do run the risk of going to a CWO who is antichoice and won’t give you the payment.
Other women have sold items on ebay to fund their terminations, or borrowed smaller amounts from various siblings or friends. You might have some coins in an old jar that you can put towards it. Maybe you have a fiver in an old coat. Or a €20 left in an old Post Office account. Withdraw it. Depending on your circumstances and ability to travel, you could be looking at paying anything between €450 and €2,500 to travel overseas to have a termination. Remember that the Abortion Support Network can give advice on the least expensive way to arrange your abortion and travel in addition to providing financial assistance to those who can’t afford to travel.
The medical abortion (abortion pill) costs less if you’re ordering it online, around €80, but you can only do this up to 10 weeks gestation. Surgical abortions will cost more but it will be cheaper if you do it without anaesthetic. Abortion is available in Britain on a broad range of grounds up until 24 weeks gestation. After 24 weeks, abortion is only permitted in Britain to save a woman’s life or prevent serious permanent harm to her physical and mental health; or where a child is likely to be born with a serious physical or mental disability. The later the gestation, the more expensive the procedure. Irish women usually have later abortions because it takes them longer to get the money together to travel.
If you’re reading this and not pregnant, start putting money away in a rainy day fund now. Open a credit union account if you can.
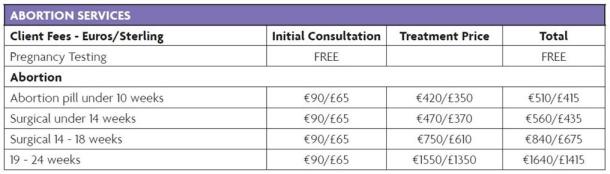
BPAS price list for those travelling from Ireland – April 2017

Travelling for your abortion
Skyscanner is useful for checking for the cheapest flights. Make sure you liaise with your clinic first so that they have an appointment time available to suit you and with ASN beforehand if you’re getting financial assistance. If you have any serious medical conditions or are later along or have a particularly high BMI, that clinic may not be able to perform the exact procedure and may need you to go to a different clinic, so make sure you’re giving them accurate information so that you can have your procedure the day you travel. Also, book your appointment before your flights because it will be easier for them to adjust your appointment time if necessary than it will be for you to change your flights if needed.
If you fly over, you will need a passport for Ryanair so budget for that. Aer Lingus will take a number of different photo id’s including a work id with your photo on, a student id or a social welfare id if you’re travelling to Britain. If you can’t get an appointment in the UK and are travelling with Aer Lingus or another airline to somewhere else in Europe, you will need a passport. You can apply for a passport here and it costs €80.
Once you get there, if you’re travelling to a BPAS clinic, they have an excellent series of PDFs that show you the transport links to clinics from the airport nearest you. NUPAS also have a free courtesy taxi service. If you’re travelling to a Marie Stopes clinic, they have a free taxi pick up service for their clients coming from Ireland. When you make your appointment, the clinic will give you directions on how to get there via public transport anyway.
Outside the clinic
When you get to the clinic, there may be protesters outside. Protesters tend to stay at larger clinics but they aren’t allowed on premises so if there’s a car park outside and you arrive by taxi, you won’t have to deal with that. This can be distressing for women but this link provides useful information. Just remember, you aren’t doing anything wrong. Don’t engage with them. Just keep walking. If you’re very concerned about it, call the clinic and explain this to them and someone will escort you in.
Inside the abortion clinic
When you get inside, don’t be alarmed by the fact there are other Irish women there. They are all there for the same reason as you. You will never see them again.
Information on the abortion treatment and procedures is available here.
The length of time you’ll be at the clinic depends on the type of procedure you’re having but it will be anything from 3 hours to an overnight stay. For example, if you’re having a surgical abortion up to 14 weeks it takes around 15 minutes with an hour of recovery time. If you’re having the abortion pill and you’re under 9 weeks you can take both tablets in one go, but over 9 weeks and you’ll have to take one tablet and then come back in 1-3 days (this is why having an accurate knowledge of gestation is so important), and of course staying longer will increase the cost of your stay in Britain. 10-14 women travel to Britain every day from Ireland for abortions and most of these go over and back on the same day.
Consider when you’re paying if you want to do it by cash or debit card. Most clinics won’t have the name of the clinic show up on the card but you can check with them in advance in case you’re concerned. Depending on the exchange rate that day, it could be cheaper for you to pay in cash with sterling.
If you need accommodation, the clinic you attend can probably send a list of reasonably priced B&Bs if you ask them. If you can’t afford accommodation, contact Abortion Support Network. Abortion Support Network do not provide accommodation for women having Early Medical Abortions.
If you need to account for being away for a day or two, you can say you were just going on holiday or that you had a job interview. Try to keep things simple. Remember that there is no shame in your abortion, you have done nothing wrong – regardless of whether you choose to tell people or not. If you would usually bring your Aunty Pat a fridge magnet from your holiday, and you’ve told her you’ve gone on holiday, try and do the same this time.
Travelling for abortion after 24 weeks
If you need an abortion after 24 weeks because of a serious foetal condition, you may have to go to a specialist clinic for this. There are a few hospitals England that will provide the necessary treatment but you may have to wait a few weeks for an appointment. Depending on the stage of pregnancy and your medical requirements, the procedure may differ so it is best to speak directly to the hospital about the costs. In some late term abortions, the procedure is that the foetal heart is stopped and then the foetus is subsequently delivered. What some women have found in Ireland is that it costs around €1,500 for the first part and another €1,500 for the delivery so they opt to travel the first part done in Britain, and then return home to deliver the foetus in an Irish hospital where they have the support of their family. This also removes the cost of transporting foetal remains home to Ireland for burial. Some women simply prefer this option. Please do not be alarmed by these figures. Liverpool Women’s charges around £1634 for the whole procedure including the stay at hospital with your partner and it really depends on your particular needs.
If your pregnancy has been diagnosed with a fatal foetal anomaly, you are not alone. You can contact AnteNatal Results and Choices (ARC), a UK charity helping people understand their diagnosis and providing information. You can also contact Termination For Medical Reasons, a group in the Republic of Ireland made of women and couples who have made the trip to England to terminate pregnancies for medical reasons. They have a support group called Leanbh Mo Chroi – 086 3745474 or leanbhmochroi@gmail.com.
If you are in care….
If you are in residential or foster care, you have the right to travel to access abortion services. Contact your social worker to make these arrangements for you. Be aware, that in many cases where young people in care have attempted to seek abortions overseas, they have had to go through psychiatric assessments with the HSE and there have been court hearings.
If you need a visa to travel…..
If you are an asylum seeker, there is provision for you to get travel documents to access abortion overseas but it is an arduous process. You solicitor can also seek funds from the HSE via court order to assist you with the cost of travelling. You can contact the IFPA for more information on getting the assistance to travel from the HSE. As outlined here, you will need two visas, one to leave Ireland and one to make sure you get back in. If English is not your first language, let them know when you are booking your appointment, in many cases, a translator can be provided.
If you are a migrant or a refugee the best places to go if you need a visa to travel are:
MRCI Migrants Rights Centre Ireland http://www.mrci.ie (01) 889 7570
IRC Irish Refugee Council www.irishrefugeecouncil.ie (01) 764 5854
The MRCI and IRC share a Dublin office.
Depending on what country you are from, it may be easier for you to get a visa for The Netherlands or Belgium.
A legal abortion in Ireland?
If there is a real and substantial risk to your life, including a risk of suicide, you may be entitled to an abortion in Ireland. This is not guaranteed. In the Ms. Y case, the young woman was suicidal but was ultimately coerced under threat of legal action to undergo a c-section at 24 weeks despite being deemed suicidal. We are aware of another case where a suicidal woman was granted an abortion though, but there are too few cases at the moment to predict how applications will be treated. If there is a risk to your life because you are suicidal as a result of your pregnancy and want to seek treatment in Ireland, speak to your GP. It may be best to make alternative plans to travel simultaneously in case your request for a termination is denied. If you are suicidal, there is a list of contacts that may be of assistance to you here.
After your abortion
When you return, you should attend for a post-abortion check up with your GP or with the IFPA or a Well Woman Clinic. Post-abortion check-ups are free as they are state funded. Post-abortion counselling is also free. A list of clinics where you can access non-judgmental counselling is here. From a doctor’s point of view, a medical abortion (an abortion using the pill) is indistinguishable from a miscarriage. You don’t have to tell your doctor about it, but there’s some useful information here and here that may help you make that decision. Be aware that if you tell your doctor you took the abortion pill illegally in Ireland, there is a chance they may report you to the authorities. Your doctor is not legally obliged to report you in the South, but doctors are legally obliged to report you in the north. It may be worthwhile travelling to access post-abortion care from a provider you know will not report you.
Take it easy. Consider your future contraceptive needs. Talk to a friend or a professional if you feel you need to but don’t feel you have to. It can be a big emotional deal even when you’re 100% confident you made the right decision. So most of all, be kind to yourself.

Budgeting for your abortion overseas – A Feminist Ire Cut Out & Keep Guide
| Cost | |
| Pregnancy tests | € |
| GP Visit | € |
| Phone credit for making calls to clinic / booking flights | € |
| Passport or ID Cost | € |
| Cost of travel documents or solicitor consultations to get them | € |
| Dating scan (optional) | € |
| Getting to ferry or airport (bus or taxi fare) or alternatively, airport parking plus petrol costs | € |
| Plane or ferry ticket cost | € |
| Plane or ferry cost for partner or friend accompanying | € |
| Phone credit for journey | € |
| Cost of printing documents (boarding pass, utility bill etc). | € |
| Accommodation | € |
| Fee for Abortion Treatment | € |
| Cost of Contraception | € |
| Food | € |
| Painkillers | € |
| Sanitary towels | € |
| Travel from clinic to airport | € |
| Travel from airport to home | € |
| Childcare fees | € |
| Miscellaneous | € |
| TOTAL | € |

